



Report Shares Lessons from Health Department-Medicaid Agency Collaboration to Improve HIV Outcomes
Topics
A new evaluation report discusses the processes and short-term outcomes associated with collaborative efforts by public health department and Medicaid agency staff in 19 states to increase viral suppression and improve health outcomes for people with HIV enrolled in Medicaid. The state teams were participants in the HIV Health Improvement Affinity GroupExit Disclaimer, a one-year activity co-led by several federal agencies that provided support to the state teams. The findings in the evaluation report may offer insights and lessons to other states seeking to engage in similarly focused collaborative efforts as well other types of cross-programmatic collaboration and cooperation.
What Was the HIV Health Improvement Affinity Group?
Medicaid is the single largest source of healthcare coverage for people with HIV and the number of Medicaid beneficiaries with HIV is increasing.Exit Disclaimer The National HIV/AIDS Strategy: Updated to 2020 called on the Centers for Medicare & Medicaid Services (CMS), the Centers for Disease Control and Prevention (CDC), and the Health Resources and Services Administration (HRSA) to form the HIV Health Improvement Affinity Group (HHIAG). The HHIAG fostered partnerships between participating state public health departments and state Medicaid agencies to develop and implement a state-specific plan focused on increasing viral suppression and improving other health outcomes among Medicaid enrollees living with HIV.
A geographically diverse group of 19 states participated in this one-year initiative (October 2016 – October 2017).

Most state plan objectives focused on strengthening data sharing and utilization between Medicaid and state public health departments, measuring viral suppression, and improving program quality. Federal partners, with support from the HHS Office of HIV/AIDS and Infectious Disease Policy, and in partnership with the National Academy for State Health Policy, offered opportunities for peer-to-peer exchange through in-person meetings, learning calls and other resources, such as webinars, a website, and individualized technical assistance.
Affinity Group Outcomes
A mixed-methods evaluation of the HHIAG support and activities identified the following outcomes:
- Data-related Outcomes: Participating in the HHIAG led to the forming or strengthening of data-sharing agreements, actual data sharing, quality improvement initiatives, and policy changes.

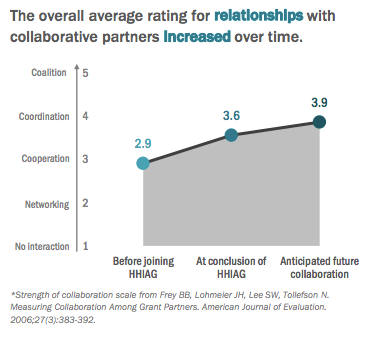
- Collaboration : Developing a shared action plan spurred collaboration between state Medicaid and public health partners that resulted in newly formed or strengthened relationships that would be sustainable.
- Knowledge: Participants became more knowledgeable about their partner agency, including their culture, priorities, policies and how to use and interpret data from each agency including surveillance and program data. As noted by one state Medicaid agency respondent, “Agencies operate differently and so it was kind of a translation type exercise to work together with HIV to be able to communicate to the Medicaid Health Plans in a way that they will digest information and seek to do something action oriented around it.”
Lessons Learned
Some of the lessons learned from the evaluation may be useful to other states and federal agencies interested in cross-programmatic collaboration.
First, participation in the HHIAG created opportunities to establish and strengthen partnerships between Medicaid and public health at the state and federal levels.
Second, the HHIAG provided a structure and environment in which participants could:
- Meet regularly and identify the unique assets available to each agency brought to the table;
- Identify, learn from, and in some cases adapt promising practices from other states; and
- Pursue high impact structural and policy changes.
Finally, prioritization of this effort by federal partners gave it credibility and helped states justify spending the time and resources on their state plan objectives.
The HHIAG was a successful model for addressing public health issues that cross agency boundaries. We encourage other similar collaborations to also include an evaluation component to further specify what works best for improving health outcomes across a wide array of conditions. (Note: the success of this approach led to the subsequent launch of a similar hepatitis C-focused affinity group that continues its work.)
If you are interested in learning more, the evaluation report [PDF, 1.1MB] and a one-page summary [PDF, 214KB]of the report are online.